You are having an operation called an Anterior Resection and this booklet aims to help you to understand your condition and this operation.
The nurses and doctors looking after you will use diagrams to help explain.
If you have any questions or would like them to go over any information again, please ask and they will be happy to do so.
We will be happy to answer your questions and talk through any worries that you or your relatives may have about your proposed operation.
If you would like an appointment please telephone 01302 644365 to arrange a convenient time.
There is a glossary at the end of this page to help you understand the terms used.
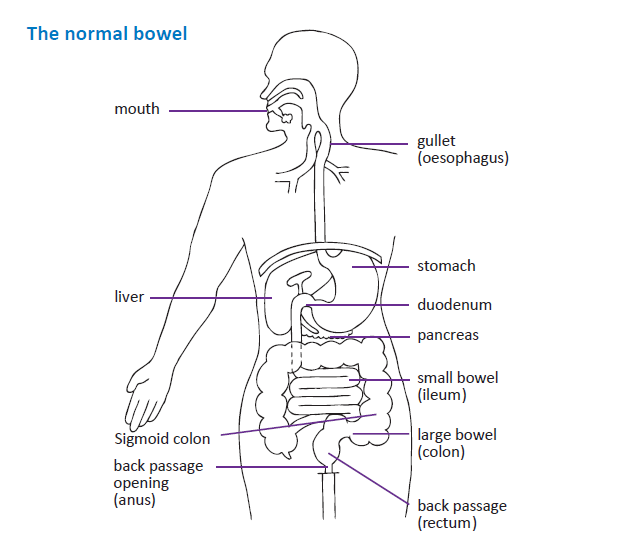
Understanding digestion
To understand the operation you will be having, it is helpful to have some knowledge of how your body works.
When food is eaten it passes from the mouth down the gullet (oesophagus) into the stomach, where it is broken down into a semi-liquid.
This then continues through the small bowel (ileum), which is a coiled tube many feet long where digestion of nutrients takes place and where most of these nutrients are absorbed into the body.
Following this the waste products (faeces) move through the large bowel (colon) into the back passage (rectum) and through the back passage opening (anus), for passing out of the body when we go to the toilet.
Why do I need this operation?
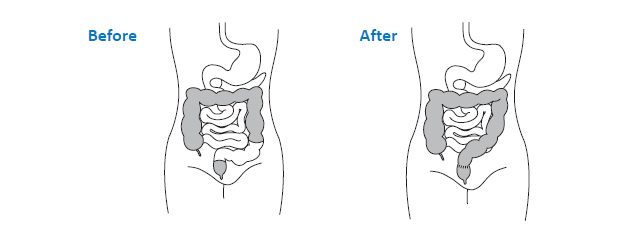
You have been diagnosed as having a cancer in the lower part of your large bowel known as the rectum (back passage). The usual treatment is surgery to remove the piece of bowel involved and join the two ends together. The join is called an ‘anastomosis’.
Depending on the position of your cancer the surgeon may decide to create an internal pouch. Sometimes it is necessary to form a temporary opening in the bowel (stoma) at the time of the operation, to divert the faeces. If this applies to you, the reasons for this will be discussed further.
Most people stay in hospital between 2 and 14 days, depending on their progress. This also depends if there are any complications of surgery. This will be discussed in more detail later in this booklet.
What is bowel cancer?
Bowel cancer is a disease of the large bowel where malignant cells grow and multiply abnormally, forming a growth or tumour which is called a cancer.
Bowel cancer is one of the most common cancers in the UK. It is usually treated by having an operation to remove it.
What causes bowel cancer?
At present the cause is unknown, although some families do seem to be more at risk of developing the disease. Some environmental factors can contribute to cancers but individual cases can not always be explained.
Will my operation cure my cancer?
Bowel cancer can be cured if it is found at an early stage. The stage that the disease has reached is determined by sending the piece of bowel removed at the operation to the laboratory for histology (examination under a microscope). Once the results of these tests are available (and those of any other investigations such as scans or X-rays), the results will be discussed by a team of experts (the multi-disciplinary team). Histology results are usually available about 2-4 weeks after the operation and any decision made on further treatment will be discussed with you before discharge or in clinic.
What further treatments may be offered?
There are many different forms of treatment for cancer. The MDT will decide whether further treatment is necessary and you will be advised regarding this. The Oncologist may decide to treat you with drugs (chemotherapy) or X-ray treatment (radiotherapy), or a combination of both. On some occasions treatment may be given before the operation. For many patients, the surgery will be the only treatment they need.
Are there any risks involved in having bowel surgery?
Most people get through their operation with no problems. However, it is important to realise that sometimes there can be difficulties.
Sometimes there are problems with the healing of the new join in the bowel. It may be necessary to create a new opening by bringing the bowel out through the tummy (abdomen), where it will be stitched to the skin – this is called a stoma. There are other information books about having a stoma and these will be made available to you.
Some patients maybe able to have their bowel operation laparoscopically (keyhole surgery). The surgeon and colorectal nurse will discuss this with you. If you have the operation by keyhole, you will have a number of very small wounds across your abdomen (tummy) rather than one long wound. However, many patients have a small incision as well. Sometimes the operation may begin laparoscopically but may have to be changed to an open procedure (when the abdomen is cut open) due to technical reasons.
Risks can include infection, which may affect the chest, ‘water-works’ (urinary tract), or the wound which is down the centre of your tummy (abdomen) in this operation.
Following the operation there is a risk that men may experience difficulties in achieving an erection. Women may find that after the operation there may be some discomfort during sex. There is a small risk in both men and women that the operation may cause problems with passing water (urine).
These problems are often temporary and may improve with time.
With any big operation like Anterior Resection, there is a small risk of serious complications such as heart attack, blood clot, heavy bleeding (haemorrhage) or, extremely rarely, there is a risk of not surviving due to problems related to the operation. Although these risks are very small it is important that you are aware of them so that you have all the information you need before agreeing to have an operation. There are other long-term complications that may arise following bowel surgery. Firstly, weakness along the scar can develop, resulting in hernia. Secondly, there is a risk of a hernia developing around the stoma, causing the area to look swollen. There is also a risk following abdominal surgery of developing adhesions (this is scarring on the inside, causing tissue to adhere to itself). This can be a long-term complication, and can sometimes result in a further admission to hospital and occasionally may require a further operation.
If you would like to talk about any of these problems in more detail, please contact the Specialist Nurse or your surgeon, who will be happy to discuss your worries with you.
What happens before the operation?
Before your operation it is important that you are as healthy as possible. You will be asked to come to a pre-admission clinic at the hospital, so that we can carry out tests to establish whether or not you have any problems such as high blood pressure or anaemia that might affect your operation.
You will have the opportunity to talk to the nurses and doctors, who will explain the operation to you. This is your chance to ask any questions you may have. Once you are sure about what is going to happen you will be asked to sign a consent form giving written permission to do the operation.
The Specialist Nurse will talk to you about the operation, as there is a risk you may need a stoma, she will mark the best position on your tummy for this.
You are likely to meet other health professionals at some stage before your operation, including the anaesthetist and the physiotherapist. Depending on the hospital at which you are being treated, you may be asked if medical students can be involved in your care. You do not have to agree to this.
Preparing your bowel
Your surgeon may request an enema or a laxative to drink, which will give you diarrhoea. This ensures that your bowel is as clean as possible before the operation. At this hospital we have a enhanced recovery programme.
The pre-op assessment nurse will explain this to you in more detail.
What happens immediately after the operation?
Some patients will need a drain, a catheter or a intravenous infusion.
As you begin to recover these will be removed.
What effects will the operation have?
Removing part of the colon need not impair good health. In the long term, however, you may experience more frequent bowel actions with loose motions. This is more common in the early period following the operation, and usually improves with time.
If your surgery involves a stoma, a Specialist Nurse will teach you to care for it. Before you go home, you will be able to manage the bag yourself. You will be given more information if a stoma is necessary to manage to care for.
Will I be able to eat normally afterwards?
Yes: because the large bowel deals mainly with waste, you will be eating normally by the time you go home from hospital, although it may be a while before your appetite returns to normal.
Everyone is affected in different ways by certain foods and your bowel may react differently to some foods after your operation.
How will I feel when I get home?
You are likely to feel tired and need to rest for part of the day, but this should improve with time. Take things gently at first, but gradually increase the amount of activity you do – try to achieve plenty of rest, gentle exercise and a well balanced diet.
Resuming normal activities
People differ, and each person will return to normal activities at their own pace. If you have any questions about this please talk to your Specialist Nurse.
Will I have to come back to hospital?
Yes: an outpatient appointment will be made for you so that we can keep a check on you after you have left hospital. How often you come back for a check-up is based on your individual needs and treatment plan. You may see either a Doctor or most likely a Specialist Nurse, for your follow up.
Sometimes you will have tests like scans or blood tests.
If you have been referred for other treatment such as chemotherapy, this may be done at your own hospital or at Weston Park Hospital in Sheffield. Radiotherapy treatment is always given at Weston Park Hospital.
Will anyone visit me at home?
Normally the District Nurse will visit you at home after your discharge.
She will assess your needs and give you appropriate care. If you have a stoma, the Colorectal/Stoma Nurse may also visit you at home to check on your progress. You will be given a contact number for the ward you were discharged from and the number for the specialist nurses is at the beginning of this booklet. You can telephone for advice or reassurance if there are any problems
or worries.
We may ask you to take part in research
It is important to find out how well treatments and care work, so we may ask you to take part in a research trial. You do not have to agree to this, and if you do not want to be involved, your decision will not affect your care. If you do agree, please remember that you can change your mind at any time during the trial.
Financial Issues
If you have financial concerns, speak with your specialist nurse who can advise you who to speak to about this.
Glossary of terms
- Abdomen – the part of the body that contains the stomach, bowel and other organs.
- Anastomosis – the surgical joining of two ends of the healthy bowel.
- Anus – the outlet of the back passage.
- Catheter – a tube inserted into the bladder to drain urine.
- Chemotherapy – treatment using drugs.
- Colon – the large bowel or intestine. It is about 1.5 metres (5 feet) long.
- Diarrhoea – abnormal frequency and looseness of stools.
- Faeces – motions, stools, waste products.
- Haemorrhage – excessive bleeding.
- Histology – examination of cells under a microscope to determine pathology.
- Ileostomy – a surgically-made opening in which the ileum is brought onto the surface of the abdomen to form a stoma. Waste is then collected in a bag attached to the skin.
- Impotence – inability to maintain an erection sufficient for sexual intercourse.
- MDT – Multi Disciplinary Team.
- Oesophagus – the part of the body that joins the mouth and stomach.
- Oncologist – doctor who is a cancer specialist.
- Radiotherapy – treatment using X-rays.
- Rectum – the back passage.
- Stoma – the part of the bowel visible on the surface of the abdomen after surgery. A bag is attached to the skin around the stoma to collect waste.
- Urinary Tract – the ‘water-works’ system.
- Urine – fluid excreted by the kidneys.
- Laparoscopically – Key hole surgery.
Content out of date? Information wrong or not clear enough? Report this page.