What is Ascites?
Ascites is a build-up of fluid in the lining of the tummy (abdomen). It can be caused by conditions such as advanced liver disease and heart failure but can also be caused by cancer or if lymph nodes in this area are blocked.
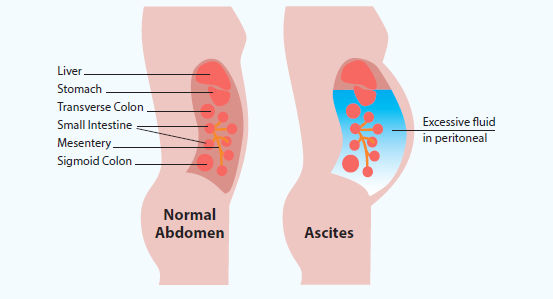
Inside the tummy (abdomen) there is a membrane called the peritoneum. It has two layers. One of the layers lines the tummy wall. The other layer covers the organs inside the tummy.
The peritoneum makes ascitic fluid, which acts as a lubricant between the two layers.
This allows the organs to glide smoothly over one another. Sometimes this fluid can build up between the two layers, in the peritoneal space. This is called ascites (See Figure 1).
Signs and symptoms
The main symptom is increased swelling or bloating in your tummy.
This may cause you to experience one or more of the following symptoms:
- pain and discomfort
- feelings of sickness (nausea)
- indigestion and constipation
- tiredness
- breathlessness
- a reduced appetite
- difficulty moving around or sitting comfortably
- swollen legs/ankles
If you have some of these signs and symptoms it is important to contact your nurse or doctor early to let them know.
They will arrange for assessment and perform any tests that are required, so that it can be dealt with before the symptoms worsen. This may include blood tests, ultrasound (USS) or Computerised Tomography (CT) scans in some instances.
Managing Ascites
Medication – These medicines help your body remove excess fluid by increasing the amount of urine you pass. This can help reduce fluid build-up and ease your symptoms.
Cancer treatments – If your ascites is caused by a type of cancer, you may be offered chemotherapy or targeted treatments, if appropriate. These treatments aim to reduce the number of cancer cells, which can help lower the risk of fluid building up in the abdomen.
Drainage of fluid from your tummy – Removing the excess fluid is a common and effective treatment for ascites. This will relieve the symptoms and allow you to feel more comfortable. This is called paracentesis.
When does it need draining?
- For symptom relief: if you are experiencing any significant symptoms that are affecting your quality of life.
- To find a diagnosis: it is possible to examine the fluid under a microscope and do special tests that might rule out cancer or tell us what type of cancer it is.
Who decides when it needs draining?
You may come into hospital as an emergency through the Accident and Emergency (A&E) department, after a clinic appointment, or after contacting your cancer team with symptoms of ascites.
A doctor or nurse involved in your care will assess you and your symptoms – either in person or over the phone – and decide whether the fluid needs to be drained.
What type of drain will be inserted?
This decision will be made by the clinical team caring for you. The options include:
1. Pigtail drain – This is usually recommended. It is used either to take a sample of the fluid (for testing) or to drain the ascites completely over several hours. The drain is normally removed once the fluid has been drained and it is safe for you to go home. In some cases, if there is a large amount of fluid, the drain may stay in place for a few days or occasionally longer.
2. Long term tunnelled drain – This may be considered if the fluid keeps coming back and there are no other treatment options available. The drain is designed to stay in place for a longer period of time. It can help reduce repeated hospital admissions and improve patient experience and comfort.
What can I expect?
Before drain insertion
The procedure will be fully explained to you along with the possible complications that may occur during and post procedure.
Following this, and once it is determined that you have fully understood all the information, you will be required to sign a consent form. You will receive a copy of this for your records.
If you haven’t had any recent blood tests, you may be asked to attend for these to be taken in the week before, or on the day of the procedure.
A referral will then be sent to the X-ray department and you will be contacted, either by phone or letter, when a date and time has been confirmed. You will also be advised at that time whether you need to omit any medication or if any other requirements are necessary.
Medication
Once a date for the procedure is arranged, if you are on any blood thinning medications (anti-coagulants or anti-platelets), you will be told by the doctor or nurse (in clinic or by phone) if this needs to be stopped and when they can be restarted.
On the day of procedure
Remember: You must bring your consent form and any medications you are taking. This includes over the counter medications.
When you arrive, you may be asked to wait while your bed area is prepared. An identification wristband will be placed on you for the duration of your visit.
Your observations will be checked, including your blood pressure, pulse, temperature, breathing rate and oxygen levels. Your recent blood test results will also be reviewed to make sure it is safe to carry out the procedure.
A member of the team will explain the procedure again, answer any questions you may have, and make sure you are happy to go ahead. You will then be asked to sign the consent form again to confirm this.
They will give you an estimated time for the drain to be inserted and advise how long you may need to stay afterwards. This is usually a few hours, depending on how much fluid needs to be drained.
During the Procedure
You will be taken to the X-ray department on your bed. An ultrasound scan (USS) will be carried out to check the amount of fluid present, as it may have reduced and drainage might no longer be needed.
Some local anaesthetic will be inserted near to the site of the proposed drain to numb the area. Using ultrasound guidance to ensure accuracy and reduce the risk of complications, the doctor will place a small drain (catheter) into the abdominal cavity (peritoneal cavity).
A drainage bag will be attached and a dressing to the drain site applied.
You will then be taken back to the ward to recover and allow the fluid to drain.
Post procedure
Your observations (blood pressure, pulse, temperature, breathing rate and oxygen levels) will be checked at least every hour for a minimum of four hours. This helps the team to identify and treat any complications as early as possible. The amount and speed of drainage will be guided by your observations and the plan agreed with the referring clinician.
You will be monitored for any pain or nausea. Please let a member of staff know if you feel uncomfortable, as medication can be given to help. You will usually be able to have drinks and a light diet after the procedure, if you feel well enough.
Your fluid balance will be recorded. This means staff will document everything you drink or receive through a drip, the amount of urine you pass, and the amount of fluid draining from the catheter. The drain site will also be checked regularly for any signs of leakage.
Depending on your condition and how much fluid needs to be drained, you may need to stay in hospital overnight or for a few days. If this is the case, a bed will be arranged for you.
On discharge
The drain may be removed before you go home, or it may need to stay in place for a little longer.
This will depend on several factors, including how much fluid needs to be drained, your general health, whether you have recently had ascites drained, and whether the procedure was carried out to obtain a diagnostic sample. The decision will be made by the referring clinician or the acute medical team.
If the drain is removed before you are discharged
Once the recommended amount of fluid has been drained, the catheter will be removed and a dressing applied. You will be monitored for at least one hour afterwards. If you are feeling well, able to eat and drink, mobilise safely, your dressing is satisfactory, and your observations remain stable, you will be discharged home with advice and dressings if needed.
You can remove the dressing after a couple of days if there is no further leakage. You may be referred to the District Nurse (DN) if the staff feel it is required.
A member of your Clinical Nurse Specialist (CNS) team will either offer a support visit prior to your discharge or you will receive a phone call to offer support once discharged to ensure you are aware of your follow up plan.
If the drain remains in place when you are discharged
Once the recommended amount has been drained, plans will be made for your discharge from hospital. The catheter may be left on free drainage, or a plan may be agreed to drain a set amount each day. This helps to prevent the fluid from draining too quickly, which can lead to complications.
You will be monitored for at least one hour before discharge. If you are eating and drinking, mobilising safely, your dressing is satisfactory, and your observations are stable, you will be able to go home.
You will be provided with a discharge pack containing the equipment you need. A referral will be made to the District Nursing team, and if you have a long-term drain, a referral may also be made to the drain company for additional support, training and troubleshooting.
All patients will be discharged with a discharge advice sheet.
Possible complications
Most people do not have a serious problem from having their ascites drained but here are some of the main ones to be aware of:
Bleeding – There is a small risk of bleeding when the catheter is inserted. This is usually minor and settles without the need for treatment.
Low blood pressure or raised pulse – This can happen as fluid is drained. Your observations will be checked regularly so any changes can be identified and managed promptly.
Infection – This is not common but as with any procedure there is always some risk of infection. Your temperature is monitored hourly and if it becomes raised this could indicate infection. This
will be explained in more detail with you prior to your discharge and included in your advice leaflet. If an infection develops, antibiotics will be prescribed. In some cases, the drain may
need to be removed and a decision made about whether it should be
replaced.
Blockage – Occasionally the drain can become blocked, preventing fluid from draining. Changing your position or sitting more upright may help.
Leakage – Sometimes there can be leakage from the site, this would usually stop once the fluid has been completely drained. The drain site will have a dressing which can be regularly changed if necessary.
Drain becoming dislodged (if discharged home with a drain) – Although the drain is secured with a dressing, it can become dislodged if pulled or caught. If this happens, contact your
District Nurse or cancer keyworker immediately. Your cancer team will assess whether the drain needs to be reinserted.
Low mood – Ascites can affect how you feel physically and emotionally, including how you feel about your body. Support is available:
- Contact your GP or District Nurse
- Speak to your Clinical Nurse Specialist or keyworker
- Ask about referral to counselling or a support group, if appropriate
- Consider complementary therapies if recommended
- If you have a supportive family and close friends, tell them how you are feeling. They can help to offer support too.
Patient Advice & Liaison Service (PALS)
The team are available to help with any concerns, complaints or questions you may have about your experience at the Trust. Their office is in the Main Foyer (Gate 4) of Doncaster Royal Infirmary. Contact can be made either in person between the hours of 9am-3pm, by telephone or email.
The contact details are:
Telephone: 01302 642764/642767 or 0800 028 8059
Email: dbth.pals.dbh@nhs.net
Content out of date? Information wrong or not clear enough? Report this page.